
At this time, the number of infections, while important, is not the overriding indicator to base policy decisions on. There are significant uncertainties surrounding the accuracy of testing and the establishment of infection numbers. These issues lead to problematic media reporting, misguided policy decisions, and a confused, fearful public.
IATF, DOH, UP, media and others are forgetting an important law in epidemiology, the science of epidemics: Farr’s Law. It states: ‘The death rate is a fact; anything beyond this is an inference’.1https://www.cebm.net/covid-19/covid-19-william-farrs-way-out-of…, an article from the Center of Evidence-Based Medicine of the University of Oxford. William Farr is considered one of the founding fathers of epidemiology. IATF = Interagency Task Force on COVID-19 (has longer name), DOH = Department of Health, and UP = University of the Philippines. The real crucial indicator to watch is the death rate or Case Fatality Rate (CFR), not infection numbers that are inferences from faulty tests.
Since 15 May 2020, with very minor variations due to erratic reporting, our death rate has been declining for over two months.2This is true despite the fact that our death figures, like other countries, are bloated. Deaths from co-morbidities are mostly included in the count of deaths from COVID-19 itself. https://swprs.org/a-swiss-doctor-on-covid-19/. Updated July 2020. We should be hopeful, not fearful.
Figure 1. Case Fatality Rate
The seeming rise of the death rate near the end of the chart is due to late reporting of deaths that took place weeks and even months before. Here are some examples.3 For July 13, 2020, source is https://rappler.com/nation/philippines-coronavirus-cases-climb-further-over-57000; for July 17, https://cnnphilippines.com/news/2020/7/17/63000-ph-coronavirus-covid-19-cases.html; for July 18, https://www.cnn.ph/news/2020/7/18/ph-covid-19-cases-65k.html; for July 19, https://newsinfo.inquirer.net/1308981/doh-reports-additional-2241-covid-19-cases-total-now-at-67456; for July 20, https://newsinfo.inquirer.net/1309368/weeks-before-july-ends-confirmed-covid-19-cases-near-70000; for July 21, https://rappler.com/nation/coronavirus-cases-philippines-july-21-2020.
On July 13, 2020, 65 deaths were reported. But only 9 deaths occurred in July. Two deaths happened in May and 54 deaths in June. On July 17, of the 17 deaths reported, only 9 deaths occurred in July. Six (6) deaths happened in June, one (1) in May, and one (1) in April. Similarly, on July 19, 2020, of 58 new deaths reported, only 25 were from July and 33 deaths were from June.
Vast Majority of New Infections Not Serious; Many Recoveries
On July 18, 2020 the Department of Health (DOH) reported 2,357 new cases placing the nationwide total of cases to 65,304. However 90% of these active cases had “mild symptoms” and 9% had no symptoms. In short, 99% of new cases were really nothing to get overly excited about.
This reinforces an earlier report by DOH when the new active cases reported were 39,593. Of this number, those with mild symptoms constituted 90.3% of the cases and 8.8% had no symptoms. Around 0.4 percent were severe cases and another 0.4 percent were in critical condition. In short, again 99% of the new cases were not serious at all.
Furthermore, by July 20, the DOH reported that 23,072 patients have recovered and only four (4) additional deaths occurred. And, on July 21, the DOH reported 1,951 new cases, bringing the total cases to 70,764. Yet only two deaths occurred and recoveries were up by another 209, bringing total recoveries to 23,281.
In short, the vast majority or 99% of new infections are not serious. Also, most of these cases eventually recover, constituting 32.89% (23,281) of the total cases of 70,764.
We should be deducting these recoveries as well as the deaths that have occurred from total cases. In future reports, DOH and media should also be reporting on NET total active cases and CFR. This will give a more realistic picture of the crisis.
While more accurate reporting can calm the fears of the public somewhat, it is not enough. Our analysis is not yet complete. There is a proverbial white elephant sitting in the room: defective testing which is giving us all these inflated numbers.
Low CFR and many recoveries point to a structural defect in the testing method.
The low death rates are emphasizing that the daily ritual count of infections is a case of misplaced concreteness. Whether through ignorance and hard-headedness, focusing solely on numbers of infections without a balancing context, is a masochistic way to scare the nation endlessly.
Existing tests are notoriously defective. This is the reason for so many false positives. Asymptomatic individuals are another indication of this. This is worsened by the reality that a) doctors and scientists have no consensus on what constitutes the symptoms of the COVID-19 disease and, b) scientists, until now, have not isolated the causative virus. And worst of all, Nobel Prize winner Kary Mullis, the inventor of the PCR, the core basis of the RT-PCR tests used all over, warned repeatedly that his invention should not be used for diagnosis of viral diseases. It is prone to large mistakes.4COVID19 PCR Tests are Scientifically Meaningless – OffGuardian at https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/ . See also https://covidcalltohumanity.org/faulty-covid-19-tests-why-prisoners-love-their-jailers-and-never-ending-lockdowns/
In addition, positive test results do not automatically mean that someone is truly infected with the virus. Yet, once someone is test-positive, almost everyone believes that the test-positive individual is infected, and then subjected to all kinds of quarantine procedures. Test-positive does not mean infected. The declining CFR reflects this.
Figure 2. Test Rates and Positive Rates5Figure 2 created using official government data.
Figure 2 points to the scientific uncertainty of the tests. The increasing infection numbers may be due more to the increasing numbers of defective tests. Starting from 02 June to 16 July 2020, when the government started testing anywhere from 10.000 to around 25,000 tests per day, the percent of test-positive individuals per batch of total tests for the day varies within a specific narrow range of 4 to 14%.
Assuming, for the moment, the government data is accurate, you will note the very interesting association between the increase in tests and the increase in test-positive individuals. When the number of tests increases or decreases per day, the number of test-positive individuals also increases or decreases per day, respectively. This is true for an overwhelming number of days.
The ratio between test-positive individuals and the number of tests should vary more widely and erratically, reflecting the variability and randomness in the characteristics of the general population. For example, young people are mostly not affected by the disease. Yet they are testing positive and then nothing really happens to them.6See reference 3 above and Table 2 below. Furthermore, as more tests are done and assuming there is a real epidemic happening, then the percentage of test-positive persons should be increasing.
One way to determine the accuracy of this testing process is to subject it to randomized sampling. When Iceland did these nation wide randomized tests, the results showed only 0.3%-0.8% of its population is infected with the COVID-19. And equally revealing, of those who were test-positive, around 50% were asymptomatic.7https://www.usatoday.com/story/news/world/2020/04/10/coronavirus-covid-19-small-nations-iceland-big-data/2959797001/ These results hold stark lessons for the Philippines.
Vast Majority of Test-Positives Coming From Safer Age Groups
To further ease concerns about high infection rates in the Philippines, take a look at the demographic profile of Test-Positives in Table 1 and Table 2 below.8Tables 1 and 2 are taken from an important COVID-19 statistics tracker made by the Gonzalo siblings in the Philippines. See their website here: https://covid19stats.ph/stats/by-demographics These are based on the SARS-CoV-2 tracker of the Department of Health (DOH). The figures are for July 20, 2020 when cases reached 68,898.9The Philippine Daily Inquirer reported 69,898 for this day. https://newsinfo.inquirer.net/1309368/weeks-before-july-ends-confirmed-covid-19-cases-near-70000. For sure, this is due to data adjustments on either side. But since Tables 1 and 2 are based on reference 7 above, the figure of 68,898 is used to illustrate a very important point that minor differences will not alter.
Table 1 shows that 78.1% of the new cases are from individuals aged 20-59 years old. The senior citizens, or those above 60, together constitute only 13.6 % of the new cases. This is very encouraging news because the cases from ages 20-59, which compose most of the cases, have a high probability of being safe. We can see this clearly in Table 2.
Table 1. Demographics of COVID-19 Cases by Age Group
Table 2. Demographics of COVID-19 Fatality by Age Group
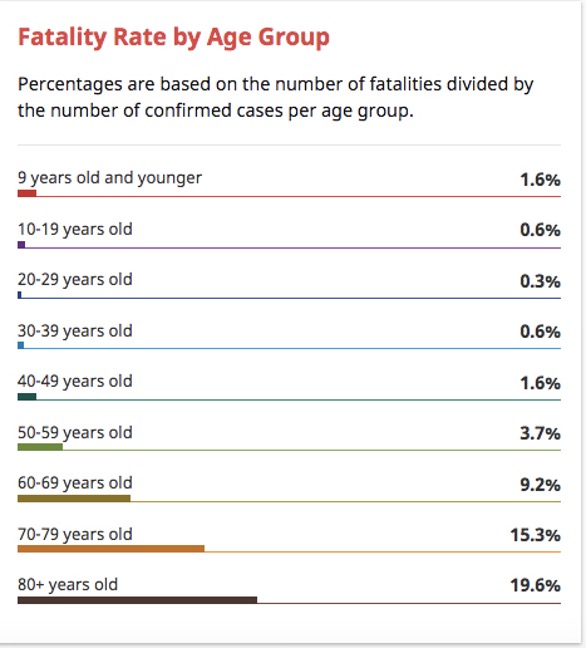
This is not to say that it is fine for elder people to die. The real message here is to focus on the elderly and the more vulnerable segments of the population. And then we have nothing to fear from the perfect storm of the use of defective tests, automatic assumption that test-positive equals infection, and the mistaken belief that infection means high chance of dying.
The Philippine susceptibility by age group converges with the global experience10Note that Table 2 above is based on the CFR or the Case Fatality Ratio. The Ioannidis study is based on IFR or Infection Fatality Rate. The IFR is a more precise measure than CFR. As already discussed above, test-positives are not necessarily infected cases. But CFR is based on test-positives. The IFR, on the other hand, is based on actual confirmed infections, using antibody tests, not just test-positive cases using RT-PCR. It is estimated that the global CFR is around 3% and the Philippines is now below this. The IFR is much lower by around 1000 times than CFR. Of course, this will vary from country to country. On this basis, the Philippine CFR figures, if roughly converted to IFR figures, would be roughly similar to the numbers in the Ioannidis study or may even be lower given the existing demographics of a younger Philippines. https://reason.com/2020/06/28/cdc-antibody-studies-confirm-huge-gap-between-covid-19-infections-and-known-cases/ as can be seen from this study by Dr. John Ioannidis, head of disease prevention at Stanford University.
‘0.05% to 1% is a reasonable range for what the data tell us now for the infection fatality rate, with a median of about 0.25% … The death rate in a given country depends a lot on the age-structure, who are the people infected, and how they are managed. For people younger than 45, the infection fatality rate is almost 0%. For 45 to 70, it is probably about 0.05-0.3%. …. For those above 70, it escalates substantially, to 1% or higher for those over 85. For frail, debilitated elderly people with multiple health problems who are infected in nursing homes, it can go up to 25% during major outbreaks in these facilities.’11https://articles.mercola.com/sites/articles/archive/2020/07/14/coronavirus-death-curve.aspx
Avoiding Panic and Wrong Strategies based on Illusory Infection Numbers
Gerd Bosbach is professor emeritus of statistics, mathematics and empirical economic and social research. He is also the author of the book, Lying With Numbers. His view on this false picture of infections is particularly instructive.
‘The tripling of the tests resulted in a little more than tripling the number of those who tested positive. This tripling was presented to the citizens as a tripling of the infected …. Far-reaching decisions require secure foundations. This is exactly what has been neglected so far. The repeated equation of the number of positively tested people with the number of infected clouded the view’. [Emphasis added.]
The propensity of government to use the numbers of infections to decide whether to lift the lockdown or not ‘has nothing to do with reality. [We] keep talking about infected people instead of [test-] positive people. The high numbers remain in memory … And that creates fear …’
‘We should ensure that the media do not use the power of images to generate emotions that influence our judgment. If you get pictures of coffins and death departments from Italy or pictures of completely empty shelves, then their effects exceed the facts mentioned.’12Ibid.
Epidemic Coming to an End?
The figures above indicate that the epidemic may be coming to an end and normality is around the corner despite all the noise around high test-positive results. If government and media do not have the courage to face the facts and insist on their harmful sensationalistic coverage and science-deficit decision-making, they will continue misleading and harming the public.
We all need to resist falling into this trap for hope is clearly on the horizon. Instead we should demand better data and precise care management, transparency and facilitating the emergence of collective intelligence in the nation. We should call on government to desist on intimidation and scare tactics that are totally out of character given the current status of soon-to-be non-epidemic nature of COVID-19.
From media, we should demand that it upholds its real mission: Uphold objective truth and engage in fearless investigation to discover this truth. It should not mesmerize itself and the general public on constant fear mongering with news stories that need to be carefully balanced by ensuring that a diversity of constructive perspectives are reported.
Resources
- 1https://www.cebm.net/covid-19/covid-19-william-farrs-way-out-of…, an article from the Center of Evidence-Based Medicine of the University of Oxford. William Farr is considered one of the founding fathers of epidemiology. IATF = Interagency Task Force on COVID-19 (has longer name), DOH = Department of Health, and UP = University of the Philippines.
- 2This is true despite the fact that our death figures, like other countries, are bloated. Deaths from co-morbidities are mostly included in the count of deaths from COVID-19 itself. https://swprs.org/a-swiss-doctor-on-covid-19/. Updated July 2020.
- 3For July 13, 2020, source is https://rappler.com/nation/philippines-coronavirus-cases-climb-further-over-57000; for July 17, https://cnnphilippines.com/news/2020/7/17/63000-ph-coronavirus-covid-19-cases.html; for July 18, https://www.cnn.ph/news/2020/7/18/ph-covid-19-cases-65k.html; for July 19, https://newsinfo.inquirer.net/1308981/doh-reports-additional-2241-covid-19-cases-total-now-at-67456; for July 20, https://newsinfo.inquirer.net/1309368/weeks-before-july-ends-confirmed-covid-19-cases-near-70000; for July 21, https://rappler.com/nation/coronavirus-cases-philippines-july-21-2020.
- 4COVID19 PCR Tests are Scientifically Meaningless – OffGuardian at https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/ . See also https://covidcalltohumanity.org/faulty-covid-19-tests-why-prisoners-love-their-jailers-and-never-ending-lockdowns/
- 5Figure 2 created using official government data.
- 6See reference 3 above and Table 2 below.
- 7
- 8Tables 1 and 2 are taken from an important COVID-19 statistics tracker made by the Gonzalo siblings in the Philippines. See their website here: https://covid19stats.ph/stats/by-demographics
- 9The Philippine Daily Inquirer reported 69,898 for this day. https://newsinfo.inquirer.net/1309368/weeks-before-july-ends-confirmed-covid-19-cases-near-70000. For sure, this is due to data adjustments on either side. But since Tables 1 and 2 are based on reference 7 above, the figure of 68,898 is used to illustrate a very important point that minor differences will not alter.
- 10Note that Table 2 above is based on the CFR or the Case Fatality Ratio. The Ioannidis study is based on IFR or Infection Fatality Rate. The IFR is a more precise measure than CFR. As already discussed above, test-positives are not necessarily infected cases. But CFR is based on test-positives. The IFR, on the other hand, is based on actual confirmed infections, using antibody tests, not just test-positive cases using RT-PCR. It is estimated that the global CFR is around 3% and the Philippines is now below this. The IFR is much lower by around 1000 times than CFR. Of course, this will vary from country to country. On this basis, the Philippine CFR figures, if roughly converted to IFR figures, would be roughly similar to the numbers in the Ioannidis study or may even be lower given the existing demographics of a younger Philippines. https://reason.com/2020/06/28/cdc-antibody-studies-confirm-huge-gap-between-covid-19-infections-and-known-cases/
- 11
- 12Ibid.
Feels calming to know that this virus is weakening and coming to an end
whenever I ride in a taxi I used to ask the driver if there are cases of covid in their area. their answer was “namatay sa diabetis, pagdating sa ospital namatay sa covid. Sa Barangay gulod negosyante na heart attck namatay sa palengke. ang heart attack naging namatay sa covid
Thanks Sir Nick for this great news.
This is to CONFIRM on what’s REALLY HAPPENING.????????
I very much admire the objective and comprehensive depth of Nicky Perlas’ essay and the hopefulness too that it imparts.
I find this comprehensive and enlightening. Dapat talaga basahin nang maige ang data at bigyan ito ng tamang report. It seems that till now the panic and fear that we earlier on feel about the virus are sustained instead of being assuaged.
Hindi ko maintindihan. Even if we have zero deaths if local transmissions continue to grow, how can we say the epidemic is coming to an end? The same RT-PCR tests are used abroad and some countries (vietnam, thailand) already have zero local transmissions. I think that is also our goal that is why we continue to conduct these tests, to see how we are doing against our objective which ia to have zero local transmissions.
a lot of facts shows the possible control of the Pandemic & the unscientific protocols being adapted is obvious. I don’t believe that it will just end, masking & distancing will end this eventually if not the ” vaccine” when it comes.
The demographics presented could be more helpful if data number of covid cases per age group over total population per age group. This will show behaviour of each age group which needs more control. Also another table cases per location per age group.
Great insights, the only thing that you missed is the 20-59 are tested positive because they are active and normally accumulates more toxins in the bodies. And human cells normally excretes corona viruses to dissolve this toxins and excretes it thru body sweats, sneezing, coughing and via phlegm. The human corona virus residing in the nasal area was identified in 1965 and called B814 corona virus.Thats why they swabbiing deep into the nasal area to make sure they can get its fragments. Human had other corona viruses normally excreted in the lungs when there are toxins because human corona viruses acts like solvent dissolve toxins. This is the reason of false positive test in RT-PCR because they can mistakenly identified similar genetic sequence of human corona virus to the imaginary Sars-Cov-2. Bottomline we are all being played, its time to Wake up and demand an autopsy records, a proof showing they saw Sars-Cov2 in the deceased patient lungs in its wholeness not simply a fragments of genetic sequence. Isolation and purification to properly identify the Sars-Cov2 can be done, they have no excuse because they are more advance today than the 70’s who had identified viruses using electron microscopy.
Thank you for this critical detail – what is most disturbing is what happened to investigative journalism on National Public Radio stations as far as your knowledge and why do they continue the display worldwide? It smells like “Something rotten in the state of Denmark…”!!!! Any insights on that, without impugning yourself?
Nice read!
Nick offers many evidence-based information, but I feel we should be wary about lullIIng Filipinos to a false sense of complacency. Our home and societal set-up, the way it stands in the Philippines, make it difficult to protect the “most vulnerable” without the need to protect the “less vulnerable”. Just think of how poor, urban communities are structured. I think of 10 people living in a cramped space. Even if just 1 person is deemed vulnerable, can we protect the “1” without worrying about the “9”? I think of “vulnerable people” not having enough livelihood and health support from govt, forcing them to go out to make a living. I think of people with existing medical conditions who cannot get access to treatment (or valid testing), and yet do not have options to isolate. I think the challenge with the Philippines, especially with cities like Manila or Cebu, is that most of our public systems and social structures simply make it difficult to protect the most vulnerable. This pandemic has exposed our country’s collective failures to build an effective, inclusive and caring society. And clearly we cannot rely on the government, so it’s up us the citizenry to help each other and protect the “most vulnerable” by doing our part. Until we actually get to a place where Data shows the virus is truly contained, I feel it is very dangerous to even hint that we should be hopeful.
I concur with your statement Sir.
Kakaiba ngayon. Halos(repeat: HALOS) ang mga namamatay ngayon ay namatay dahil sa Covid 19. Wala na bang puedeng mamatay na ang dahilan ay HINDI Covid naman? Bakit atat na atat(kung sinuman yun) na ang DAPAT na Cause of Death ay Covid 19 virus? Hindi ba puedeng ang basehan man lang ay isang laboratory result ng throat swabbings ng namatay ay maipakita sa pamilya ng pumanaw nilang mahal sa buhay?
Comprehensive analysis of data. Kudos po sa inyo!
Coming from your presentation, 3 questions comes to mind: What is there to say that the number of deaths in July will not be mostly reported late like in previous months? Why not have a separate graph to reflect when the death actually occured? What is the trend of symptomatic cases?
Not until there are no reported deaths and increasing numbet of infections will I believe that there is truly no need to worry. As you said numbers can lie, so is reporting of cases and the non inclusion of those who died undiagnosed.
Yes, I agree that we shouldn’t panic, but the article could give a false sense of security because it’s incomplete.
It does not touch on:
– False negatives which, I assume, would be as prevalent as false positives and more dangerous;
– death rate has gone down (a global trend) because we have learned of better ways to treat the severe/critical cases…but that doesn’t mean that it’s less dangerous; and
– does not define recovery…I’ve read that one does not fully recover.
We all need optimism at this point but I’d rather err on the side of caution without panicking…
I believe in everything that I read about your article. Please let us inform every Filipinos about the truth of this covid19.
A human being has far more bacteria and viruses residing in the body than its natural cells. Bacteria & viruses that help maintain the human body’s health. A person has 37.2 trillion cells comprising its body, 372 trillion bacteria, & 380 trillion viruses residing in its body including different strains of coronavirus. Scientists know little about the functions of these invisible inhabitants. But we know about good bacteria helping assist one’s health. Scientists guess that there is a working relationship between bacteria & viruses that help overcome diseases. Thus supporting a person’s natural immune system. Vaccines destroy one’s natural capacity to fight disease. All media generated fear propaganda are promoted by Big Pharma salivating for billions in vaccine profits. Big Pharma vaccines are legally liability-free, not responsible for brain damage, autism, or death in the person vaccinated. Profits, not health, are the primary objective. Fear, panic, and herd stampede are the means to public demand for vaccines as mythical savior, but real profits for Big Pharma. As Barnum once said: “Never give suckers a break.”
I agree with you, 100%. Thank you Mr. Perlas for an objective, factual, comprehensive and scientific analysis of the current situation in Ph. I’ve heard a number of Pinoy doctors saying the same. Epidemiologists and Virologists abroad echos the same sentiment but for some reason are being censored. I wonder why.
I am with you on this reply. My question for Dr. .N icanor Perlas is wow whoever has the profits for gadgets for online classes already amassed a windfall. will a resumption of classes be feasible? say after six months?
there should be a multi-disciplinary team studying the numbers of covid 19 related cases…and PUT THEM IN CONTEXT like this report. Thank you for the sober update, Dr. Nic. Perlas!!!
Why is analysis in this manner not being discussed by the IATF? OR BY THE DOH? Data mgt and solid analysis appear to be the key issues in this so called Coronavirus pandemic mgt of the GOP. Sad..
When will the politicization of almost anything ever end in my PILIPINAS KONG MAHAL???
Very educational n informative
Thank you very much for this.
I work in a hospital. Always full of SICK symptomatic COVID19 cases testing positive. A few healthcare workers are contracting the disease and are ill.
So it’s NOT SIGN OF THE END OF PANDEMIC IS NEAR. There is genetic evidence of mutation that made the virus in Philippines becoming more infectious. In the same play of numbers that relative to more tests, more will turn positive. I will also add more are truly getting TRULY SICK. Low Case death rate have many potential reasons that needs careful evidence for each hypothetical cause. But one of them is actually badly sick patients can’t be accommodated in filled hospitals leading to late consult. Many “dead-on-arrival” or DOA patients are never labeled COVID19 but could have it and never counted as victims of pandemic.
The more important message IS: Don’t panic BUT we’re in a pandemic and we have ROLES to play so we can’t see the end sooner than later. We need more FOLLOWERS than “intelligent” analysts and experts. There’s evidence that what WHO, DOH, IATF & most local government is preaching & enforcing is effective — WEARING MASK, PHYSICAL (SOCIAL) DISTANCING, HAND & RESPIRATORY HYGIENE, QUARANTINE & ISOLATION, APPROPRIATE TESTING WORKS. YES THEY WORK!
So, let’s not panic So we can do what’s right. But DO WHAT’S RIGHT!
Excellent article. Incisive and informative. Should be a “must” reading for IATF people.
Nice read but at the end of the day infections pa rin un that can lead to death.
Great insights, the only thing that you missed is the 20-59 are tested positive because they are active and normally accumulates more toxins in the bodies. And human cells normally excretes corona viruses to dissolve this toxins and excretes it thru body sweats, sneezing, coughing and via phlegm. The human corona virus residing in the nasal area was identified in 1965 and called B814 corona virus.Thats why they swabbiing deep into the nasal area to make sure they can get its fragments. Human had other corona viruses normally excreted in the lungs when there are toxins because human corona viruses acts like solvent dissolve toxins. This is the reason of false positive test in RT-PCR because they can mistakenly identified similar genetic sequence of human corona virus to the imaginary Sars-Cov-2. Bottomline we are all being played, its time to Wake up and demand an autopsy records, a proof showing they saw Sars-Cov2 in the deceased patient lungs in its wholeness not simply a fragments of genetic sequence. Isolation and purification to properly identify the Sars-Cov2 can be done, they have no excuse because they are more advance today than the 70’s who had identified viruses using electron microscopy.
Very Factual and logical indeed. It assures us that we should not panic and that we can move on woth our lives.
However, even with this informative assurance of the real scenario , we shoild still continue to practice preventive protocols like weafing masks, social distancing and washing of hands as our new Normal.
Agree 101%. Thanks for this!
I think the article is over optimistic and draws wrong inferences from the information presented.
Case fatality rates is going down due to expanded testing. Initially we had very limited test capacity and protocols dictated that only symptomatic individuals be tested. This was applied prior to and during most of the ECQ period.
To prevent the spread of the virus due to asymptomatic individuals, testing extended to asymptomatic OFWs returning from abroad, frontline workers, and private sector employees coming out of lockdown as ECQ was relaxed.
Due to the expanded testing CFR expectedly goes down, but CFR is not going to go down to zero as seen in other countries. Thus if infection numbers continue to climb, even a low CFR will amount to a significant number of deaths.
Just as an exercise, imagine if we become lax and no precautions are taken. With a highly infectious dissease, lets assume that perhaps 1/3 of the population will be infected. With a CFR of just 1.0%, a total Phil. population = 110mil., 1/3 of population infected = 36 million, total deaths = 360,000. If CFR is onlh 0.1%, we still expect 36,000 deaths.
Another important statistic not covered is hospital bed capacity for COVID patients. Recently a lot of the hospitals have declared reaching full capacity in Metro Manila. Once the hospitalization capacity is exceeded, the death rate will probably go up as patients are not provided with critical care they need to survive.
Let us not be paranoid, but let us not be lax either. I think it is important to flatten the curve, stop increasing infections. Even if most of the healthy and young won’t die of covid, letting infections go unchecked will sacrifice the vulnerable in our population – the sick and the old.
I support you all the way. I’ve been saying from the beginning that this is a MILD and highly contagious disease. Nothing new from existing diseases which are actually more dangerous overall. And medical intervention isn’t going to improve the situation if they don’t have a change of paradigm like exercise and most of all naturally available intervention which is cheap, readily available and is strangely being refused by the institution that professes to protect humanity
Thanks for a very informative details about n-cov so that the people may not be panicking. we should be very careful and be aware nowadays to avoid the virus. Thanks so much.
On a different perspective, I quote from an blogger:
What about the people who survive?
For every one person who dies:
19 more require hospitalization.
18 of those will have permanent heart damage for the rest of their lives.
10 will have permanent lung damage.
3 will have strokes.
2 will have neurological damage that leads to chronic weakness and loss of coordination.
2 will have neurological damage that leads to loss of cognitive function.
https://www.quora.com/How-can-a-disease-with-1-mortality-shut-down-the-United-States/answer/Franklin-Veaux
I cannot vouch for the veracity of his numbers. Instead, do we have anything about how the numbers look like with those conditions similar to the above?
Is it really all about the death rate though? What about the risk of getting hooked up to a ventilator? What about long term damage to lungs, liver, kidney and brain? Also, no age group is really immune. Which kid’s life are you willing to risk? I agree that people shouldn’t panic but we also shouldn’t be complacent. I would rather err on the side of caution.
Your reflections sir is great. I also am a professor teaching on the topic evidence based policy development. Numbers really provide a clear picture of something. But not all numbers. What I always see on TV is number of COVID cases rising. The reporter just give emphasis on these numbers but on recoveries and declining death. Reporters may not have the competence to interpret and analyze data. I am happy to note of your analysis of data. DECLINING DEATHS and INCREASING RECOVERIES.
If we swallow everyday stated above, why is it that ICU beds for Covid are already full in hospitals in NCR?
I post a rejoinder here: https://docs.google.com/document/d/1IZKduAQQlQ07pjHA8KeVrpZDY2gOi-hLYSq8PLGzeB8/edit?usp=sharing
Excellent reply. Thank you for taking the time to highlight the severe shortcomings and intellectual sloppiness in discussed article.
We need This kind news today many people are living in fear thanks you for the words encouragement and hope may God bless us and be gracious to His people…
I agree with you Jim.
I think this needs to be a answered. If there are many recoveries, how did they recovered? What medicines they take in the absence of.vaccines. what medical protocol or procedures was availed of. For the thousands of recoveries there are patterns to look at. Thank you.
Finally, a voice of reason, an oasis of light; thank you Sir Nic Perlas and your diligent staff for making an effort to awaken the masses with sensibility and optimism instead of fear and despair! As it is invariably true of anyone rightfully seeking for the root cause of our current dilemma, diving deeper into the ‘rabbit hole’ leads to even more alarming questions and issues that have far-reaching repercussions not only on the Filipino people, but more significantly, on the future of humanity. We are certainly living in a very precarious point in mankind’s history.
Something to ponder on. Not to put us on a relaxed mode as far as the pandemic is concerned, but it should at least calm us and make us consider and look at the bigger picture. Still, I believe vigilance on the side of the people is still the best weapon to this virus. Wearing masks, keeping safe distances, regular washing of hands, and avoiding crowded places as much as possible. All in all this post is truly much appreciated.
Thank you sir for enlightening us!
Sharing this to my relative &friends!
God bless you sir!
I commend the author for a very enlightening and evidenced-based article. I hasten to add however that this should not be interpreted to mean we should let go of our vigilance in protecting against infection. While CFR is indeed low, It is best to conserve the use of resources ( some scarce) than to employ it to have someone recover from infection. Hospitalisation is still beyond the means of ordinary Filipino. The downtime resulting from recovery from the virus is substantial. Not to mention that studies show significant adverse effects on health of those who have recovered. We must not let up in preventing spread even as cure is available.
Very informative. But as Mr. Perlas has stated, right and critical data are important for decision-making.
I wonder if the decision-makers bothered to look at the data he
presented here.
Its also a dangerous claim. Death rates do go go down by virtue of the high positive tests but the absolute numbers of those who have serious symptoms that may lead to death are now much higher than the past months…all hospitals in the NCR are already carefully choosing only to admit the serious cases yet there are those on oxygen waiting in the tents for admission for days on end… This is the scenario that we are trying to avoid because then eventually the absolute death numbers will go up due to insufficient care. One preventable death (especially if that person is your parent, sibling or friend)… Is worth the conservative measures to control the escalating absolute numbers. Percentages can also be an easy way to gloss over the value of 1 human life that can never be returned.
Fact check on Nicanor Perla’s article:
“IATF, DOH, UP, media and others are forgetting an important law in epidemiology, the science of epidemics: Farr’s Law.”
This is not accurate. Several media outlets reported that the DOH and other government agencies did recognize the decline in CFR.
“The good news, health officials say is despite the rise in COVID-19 cases, the country’s case fatality rate (CFR) shows a decreasing trend. Both numbers also indicate that the death rate might be reaching a point of stability.
“We will see improvement. In recent months, CFR has been around 6% and it has dropped slightly to 2%. We see two factors here — the number of people dying is decreasing and our detection is increasing”, epidemiologist Dr. DJ Darwin Bandoy said.” (http://outbreaknewstoday.com/philippines-covid-19-deaths-reaching-equilibrium-62504/).
Even given Farr’s important contributions, some of his conclusions regarding pandemics were faulty. The Center for Evidence-Based Medicine (CEBM) from where Perlas got his information wrote:
“Sometimes, even giants like William Farr, got it badly wrong.
“Farr was anticontagionist, one of those Victorian era scientists who thought that miasmata produced by sewage, rubbish and dirt were the cause of communicable disease” (https://www.cebm.net/covid-19/covid-19-william-farrs-way-out-of-the-pandemic/).
There is another problem with just limiting analysis to the CFR. Yes, it is a good sign when it is going down, but if the number of cases are spiking or rising, then the number of fatalities may also be rising. For example, if you have a case fatality rate of 6% but only a hundred cases, then only 6 people die. If you have a lower CFR of even say 2%, but you have one thousand cases, then 20 people die. So, both the number of cases and the CFR have to be taken into consideration.
“However 90% of these active cases had “mild symptoms” and 9% had no symptoms. In short, 99% of new cases were really nothing to get overly excited about.”
This is misleading. People with mild or moderate symptoms can still be seriously ill. According to the World Health Organization, mild cases are “those without evidence of viral pneumonia or hypoxia”(Clinical management of COVID-19, Interim guidance, 27 Ma7 2020, World Health Organization). Moderate cases are “Adolescent or adult with clinical signs of pneumonia (fever, cough, dyspnoea, fast breathing) but no signs of severe pneumonia.” Severe cases are those with severe pneumonia and having “severe respiratory distress.”
Therefore, anything less than severe pneumonia and requiring hospitalization would fall under mild or moderate. More recently, it has even be determined that COVID-19, while caused by a pulmonary virus, is not primarily a pulmonary disease, but rather a vascular disease. The result is damaged blood vessels and blood clots that can affect the brain and other major organs of the body resulting in death or long-term damage without any effect on the lungs (https://hms.harvard.edu/news/distinctive-features).
“Scientists, until now, have not isolated the causative virus.”
This is false. Scientists have determined and isolated the virus, technically designated as SARS-CoV-2 (https://www.medicalnewstoday.com/articles/novel-coronavirus-your-questions-answered#1.-What-is-the-new-virus?). In fact, scientists have already completed the genome sequencing of SARS-CoV-2 (https://mra.asm.org/content/9/11/e00169-20).
“Nobel Prize winner Kary Mullis, the inventor of the PCR, the core basis of the RT-PCR tests used all over, warned repeatedly that his invention should not be used for diagnosis of viral diseases.”
This information is from internet posts that were wrongly attributing statements to Kary Mullis or taking his statements out of context (https://www.reuters.com/article/uk-factcheck-pcr/fact-check-inventor-of-method-used-to-test-for-covid-19-didnt-say-it-cant-be-used-in-virus-detection-idUSKBN24420X).
When Iceland did these nation wide randomized tests, the results showed only 0.3%-0.8% of its population is infected with the COVID-19. And equally revealing, of those who were test-positive, around 50% were asymptomatic. These results hold stark lessons for the Philippines.
This is misleading. One cannot compare and contrast Iceland, a developed country with a population of 341,000 and a population density of 3 persons per square kilometer with the Philippines with a population of almost 110 million and population density of 368 per square kilometer.
Table 1 shows that 78.1% of the new cases are from individuals aged 20-59 years old. The senior citizens, or those above 60, together constitute only 13.6 % of the new cases. This is very encouraging news because the cases from ages 20-59, which compose most of the cases, have a high probability of being safe.
This is misleading. The same trend happened in the United States and elsewhere. This was not a result of the testing, but the fact that as restrictions were eased and places began to open up, the young people were going out to bars and parties and becoming infected. The infection rate of older and vulnerable people lagged behind this, but as the young people then began interacting with family members, cases and deaths among the elderly and vulnerable began to rise.
This table also does not take into consideration the age distribution in the Philippines. It more or less follows the percentage of the population distribution in the Philippines for those above 20 (and recall that those under 21 and over 65 were not supposed to go out during the quarantines). This population distribution is not taken into account in these tables.
Gerd Bosbach is professor emeritus of statistics, mathematics and empirical economic and social research. He is also the author of the book, Lying With Numbers. His view on this false picture of infections is particularly instructive.
Quoting Gerd Bosbach can also be misleading in the case of COVID-19. In an article in Der Spiegel, Guido Kleinhubbert writes:
“Over the years, shopkeepers and scholars such as Gerd Bosbach and Gerd Gigerenzer have enjoyed inducing other experts to make mistakes in thinking and scaremongering. They were often right when they calculated that health risks were lower, for example in the case of bird flu or Creutzfeldt-Jakob disease – in both cases fewer lives were wiped out than feared. With regard to the corona pandemic, however, the relativizations that have recently been heard and read seem rather cynical.
“It is quite likely that Covid-19 will hardly increase overall mortality in 2020 – partly because many of the elderly victims would have died in the coming months anyway. And it could also turn out to be true that more teenagers and young adults are likely to die in traffic this year than from Covid-19. But all of these conjectures completely hide the dramas and side effects of the epidemic, the limits of the health system and the enormous economic and social consequences. Statistics can not only open eyes – they can obviously also make people blind” (https://www.spiegel.de/wissenschaft/medizin/coronavirus-die-fatale-entwarnung-der-statistiker-a-c7ac79fb-06e4-4382-9901-3759a955e58d).